Systemic sclerosis: prognosis, digital ulcers, and follow-up
In systemic sclerosis, capillaroscopy is not a magic biomarker capable of summarizing the whole disease, but it does provide a useful reading of microvascular involvement. Capillary density, late pattern, avascular areas, and longitudinal progression have been associated with digital ulcers, cardiopulmonary involvement, and worse clinical evolution, always with nuances and limitations that should be made explicit [1, 2, 3, 4, 8, 9, 10, 11, 12, 13, 14].
- The prognostic information from capillaroscopy is stronger for peripheral vascular damage, especially digital ulcers, than for predicting the entire systemic course of disease by itself [1, 4, 5, 6, 7].
- The late pattern and density loss are repeatedly associated with greater vascular severity and higher burden of organ involvement, although they do not always remain independently prognostic after adjustment for other variables [1, 3, 8, 12, 13].
- CSURI and NEMO scores may help in selected subgroups, but neither should replace serial clinical assessment or be expected to perform equally well in every patient [5, 6, 7].
- The relationship between capillaroscopy and interstitial lung disease (ILD) or pulmonary arterial hypertension (PAH) is consistent at population level, but insufficient to use the technique as an isolated organ-screening tool [1, 2, 9, 10, 11].
- Evolution of capillaroscopy over time appears more informative than a single baseline image when the clinical objective is to assess progression of vascular damage or visceral involvement [1, 2, 3, 11, 14].
- During follow-up, repeating the test is useful when asking concrete questions: is there risk of ulcer, vascular worsening, correlation with a clinical change, or progression of microangiopathy? [1, 2].
Learning path
If you already recognize a scleroderma pattern, this unit shows what the procedure can add regarding digital ulcers, progression, and organ involvement. It is especially useful if you arrive from Raynaud's phenomenon or from scleroderma pattern, criteria, and classification.
Which prognostic questions it can answer
Prognostic capillaroscopy is useful when the question is well formulated. It does not serve every purpose equally. Its performance is better for peripheral microvasculopathy and more modest when we try to infer the global risk of systemic sclerosis [1, 2].
Recent reviews agree on the following nuance: capillaroscopic findings correlate with vascular severity and with certain organ manifestations, but this association does not make the test a substitute for cardiopulmonary screening, skin examination, or lung function testing [1, 2]. In other words, capillaroscopy adds information, but it does not replace standard organ monitoring.
Prognostically, the observations most often repeated in the literature are density loss, avascular areas, late pattern, and longitudinal pattern worsening [1, 3, 8, 9, 10, 11, 12, 13, 14]. Some studies relate these findings to digital ulcers, ILD, PAH, cardiovascular events, and mortality. It is worth emphasizing that the magnitude of association changes according to outcome, study design, and adjustment for covariates.
| Clinical question | Capillary marker that usually adds the most | Relative strength |
|---|---|---|
| Is there greater risk of digital ulcer? | Density loss, late pattern, vascular scores such as CSURI or NEMO [4, 5, 6, 7] | Moderate |
| Does the vascular phenotype seem more aggressive? | Progressive rarefaction, avascular areas, and transition to late pattern [1, 3, 8, 14] | Moderate |
| Could there be greater pulmonary or pulmonary vascular burden? | Reduced density and late pattern [1, 9, 10, 11] | Low to moderate |
| Can capillaroscopy be used as the only survival predictor? | Not reliably [1, 8, 12, 13] | Insufficient as an isolated test |
Digital ulcers and peripheral vascular risk
This is probably the area where prognostic capillaroscopy is most convincing. The association between capillary loss, late pattern, and digital vascular complications has been replicated in different cohorts [1, 4, 5, 6, 7, 14].
The 2022 SCLEROCAP study showed that a history of digital ulcer was related to a more severe capillary pattern in the same finger. In multivariable analysis, ulcer history was associated with late pattern, edema, and lower capillary density, reinforcing the idea that peripheral microvascular injury is not uniform or theoretical, but anatomically correlatable [4].
In 2026, the same consortium published the prospective follow-up of SCLEROCAP in 387 patients; 369 completed follow-up and 53 (14%) had severe progression at three years. A very simple model based on Cutolo late phase, short disease duration, and age showed reasonable discrimination, with an area under the curve (AUC) of 0.74, comparable to more complex models [14]. The practical message is interesting: a well-performed qualitative reading still retains value, even compared with more complex multivariable models.
The CSURI score was one of the best-known proposals for predicting new ulcers. Its validation showed good discriminatory performance in selected patients [5]. However, Walker's prospective real-practice study highlighted its limitations: a relevant proportion of patients could not be evaluated, reproducibility between clinicians was only moderate, and performance was worse than in the original studies [6]. Therefore, although CSURI can orient, it should not be used as the only basis for therapeutic decisions.
The NEMO score uses another approach. In 2020, Del Papa and colleagues showed that high NEMO values were associated with the presence and onset of ischemic digital ulcers [7]. Again, it is useful to enrich clinical judgment, but never to replace it.
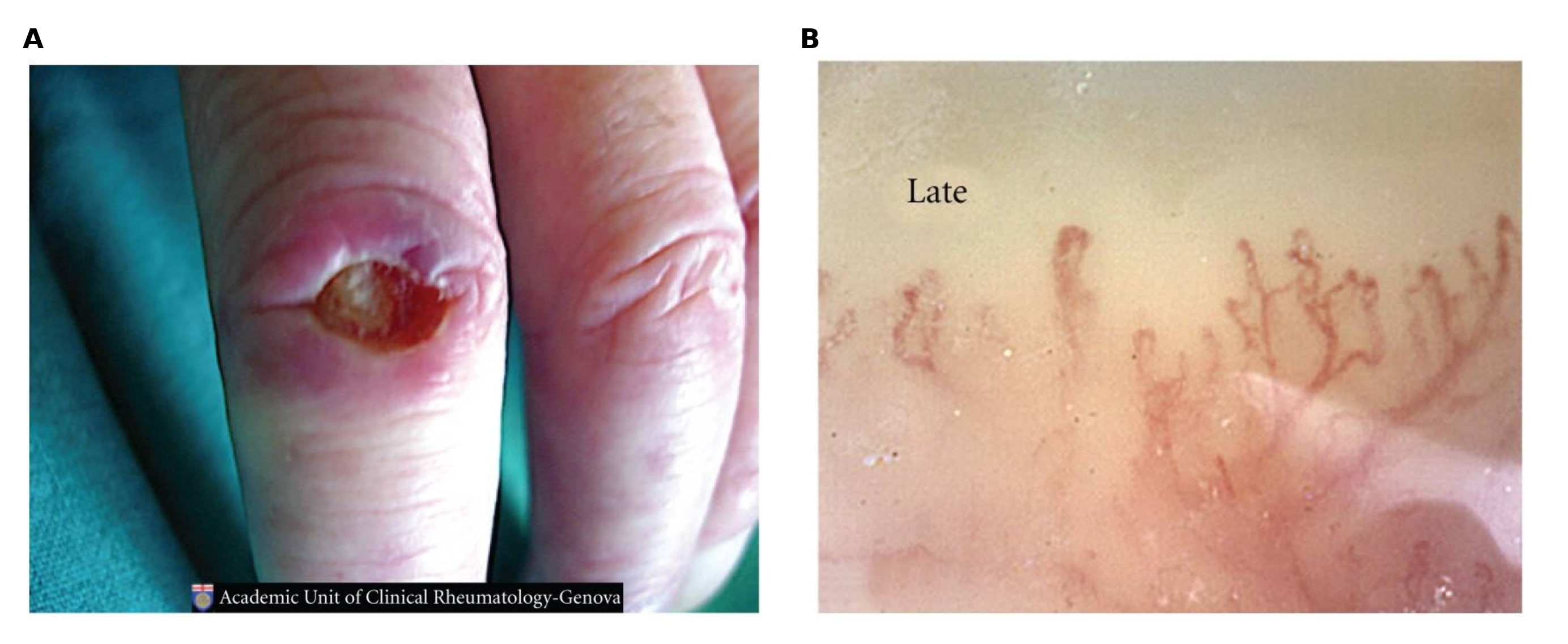
Image adapted from Cutolo M. et al., “Capillaroscopy as an Outcome Measure for Clinical Trials on the Peripheral Vasculopathy in Systemic Sclerosis,” International Journal of Rheumatology, 2010:784947, under a Creative Commons Attribution license. DOI: 10.1155/2010/784947.
| Tool or finding | What it tries to estimate | Advantage | Limitations |
|---|---|---|---|
| Late pattern / low density [1, 4, 14] | Peripheral vascular involvement and ulcer risk | Easy to integrate into clinical reading | More qualitative and observer-dependent |
| CSURI score [5, 6] | Risk of new digital ulcers | Assesses risk through a score | Not always applicable or reproducible |
| NEMO score [7] | Microvascular activity and digital ischemic risk | Captures active damage with hemorrhages and giant capillaries | Less widely implemented and requires training |
Skin, subtypes, and disease burden
The capillary pattern is also associated with the global systemic sclerosis phenotype. In general terms, late pattern and clear rarefaction are observed more often in diffuse cutaneous disease and in patients with higher burden of vascular damage [1, 8, 12].
The Spanish RESCLE cohort showed that late pattern is associated with diffuse systemic sclerosis, ILD, and scleroderma renal crisis, but did not independently demonstrate lower survival after adjustment for other major variables [8]. This is a useful lesson: capillaroscopy may reflect phenotype severity without necessarily being the strongest independent prognostic variable.
A detailed analysis published in 2025 compared limited and diffuse systemic sclerosis and found that patients with diffuse disease had greater capillary rarefaction and more severe findings, while limited disease more often showed hemorrhages and giant capillaries [12]. This helps explain why two patients with the same disease may have different images depending on cutaneous subtype and dominant phase of damage.
From a practical perspective, capillaroscopy does not replace skin scoring or serial examination, but it can reinforce the impression that a patient is accumulating greater vasculopathic burden, especially if the pattern progresses from an earlier phase to a clearly late one [1, 3, 8, 12, 14].
| Clinical feature | Described capillaroscopic tendency | Cautious interpretation |
|---|---|---|
| Diffuse systemic sclerosis | More rarefaction and higher frequency of severe patterns [8, 12] | Frequent association, but not always tied to this clinical condition |
| Limited systemic sclerosis | May show more giant capillaries and hemorrhages in certain phases [12] | Limited disease does not exclude advanced microvascular damage |
| Greater skin or vascular burden | Transition to late pattern or longitudinal worsening [1, 3, 8, 14] | Correlate with modified Rodnan skin score (mRSS) and real clinical evolution |
Pulmonary, pulmonary vascular, and cardiovascular involvement
The relationship between capillaroscopy and organ involvement exists, but here excessive confidence must be avoided. The global association is evident, but the value of the technique as a single individual screening test is much more limited [1, 2, 9, 10, 11, 12, 13].
Pulmonary arterial hypertension
A 2021 meta-analysis found that patients with systemic sclerosis-associated pulmonary arterial hypertension (PAH) had lower capillary density and more abnormal shapes than patients with systemic sclerosis without PAH [9]. In 2024, a multicenter cohort also showed higher frequency of late pattern, lower density, and more marked avascular areas in PAH cases [10]. These data are consistent, but not enough to replace echocardiography, biomarkers, or catheterization when indicated.
Interstitial lung disease
The SENSCIS subcohort published in 2025 reinforced the association between capillary loss and severity of interstitial lung disease (ILD). Patients with greater capillary loss had worse lung function and greater fibrotic extent on computed tomography [11]. Again, capillaroscopy adds an associated vascular marker, not a direct lung measurement.
Cardiovascular risk and mortality
A 2025 multicenter study found that avascular areas were associated with a higher risk of major cardiovascular events and with mortality, with adjusted hazard ratios around 2 [13]. The result is relevant because it connects microangiopathy with hard outcomes, but it remains observational. In other cohorts, late pattern has been related to a worse phenotype and lower crude survival, although the association attenuated after adjustment for age, cutaneous subtype, ILD, or PAH [8, 13].
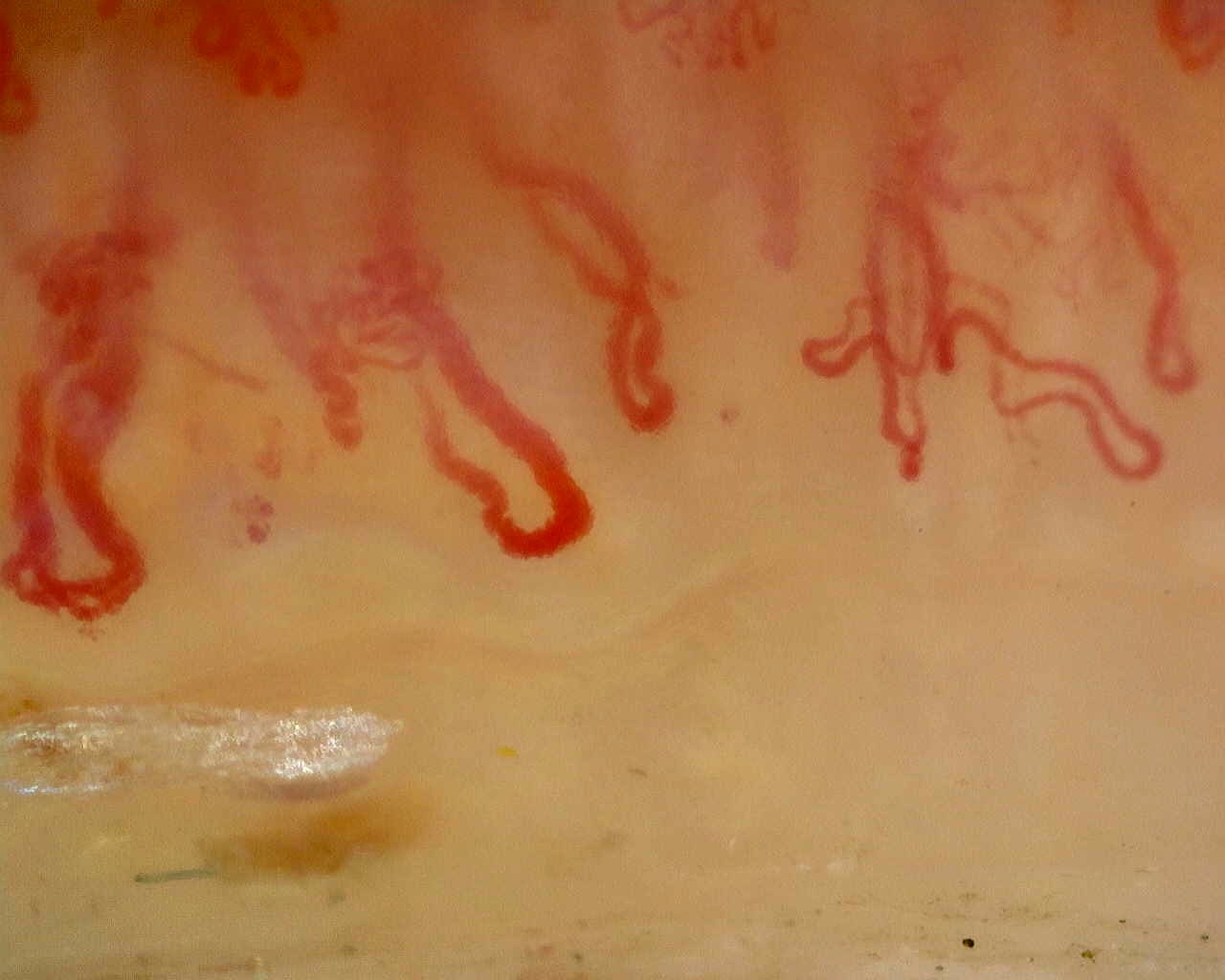 A. Rarefaction and abnormal shapes
A. Rarefaction and abnormal shapes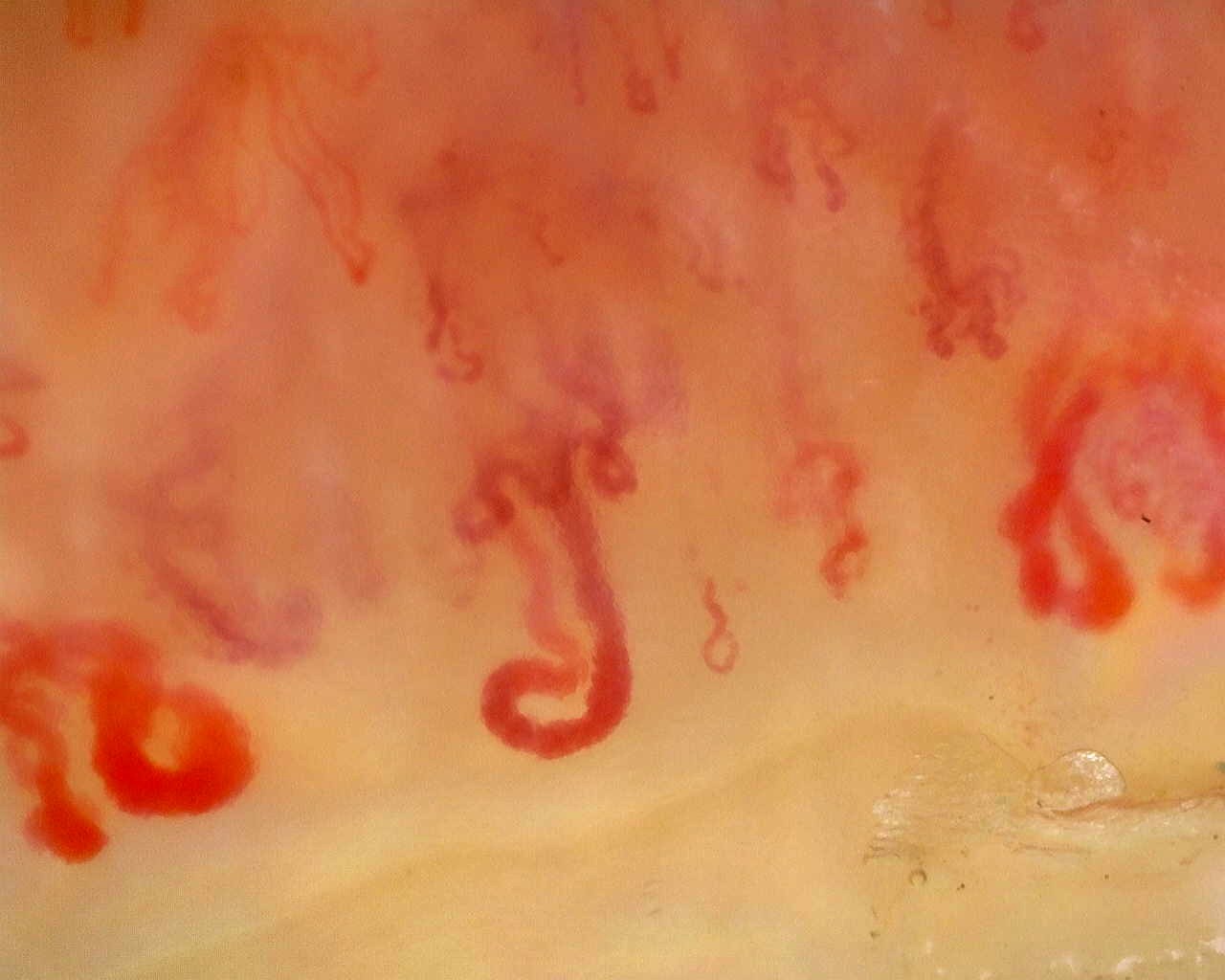 B. Avascular areas and disorganization
B. Avascular areas and disorganization| Clinical manifestation | Most repeated capillary signal | What it means in practice |
|---|---|---|
| PAH | Low density, late pattern, avascular areas [9, 10] | Raises suspicion, but does not replace cardiopulmonary screening |
| ILD | More marked capillary loss [8, 11] | Supports greater disease burden, but does not quantify the lung by itself |
| Cardiovascular events / mortality | Avascular areas and severe microangiopathy [13] | Observational association that requires context with classic risk factors |
Follow-up, repetition, and practical limitations
Repeating capillaroscopy only makes sense if longitudinal comparison can change a decision. The question is not "how often should it be repeated," but "what information do I expect to gain by repeating it."
The 2020 standardization emphasizes the importance of performing serial examinations with comparable protocols, the same fingers whenever possible, and homogeneous reading criteria [2]. If the technique changes too much from one visit to another, comparison loses value. The design of SCLEROCAP reinforces this idea well: the prognostic value of capillaroscopy was studied through standard annual assessment and serial observations, not with isolated heterogeneous images [14].
In clinical practice, repetition makes particular sense when the patient develops new ulcers, the vascular phenotype clearly changes, there is doubt about progression from a very early phase, or it is useful to objectify whether capillary rarefaction is worsening [1, 2, 3, 14]. In stable patients with already resolved clinical questions, indiscriminate repetition adds less value.
There is not enough evidence to recommend one universal interval applicable to every patient with systemic sclerosis. The reasonable approach is to adapt repetition to the context: more frequent if the vascular phenotype changes or if the result could modify follow-up, more spaced if disease is stable and the additional information is predictable [1, 2].
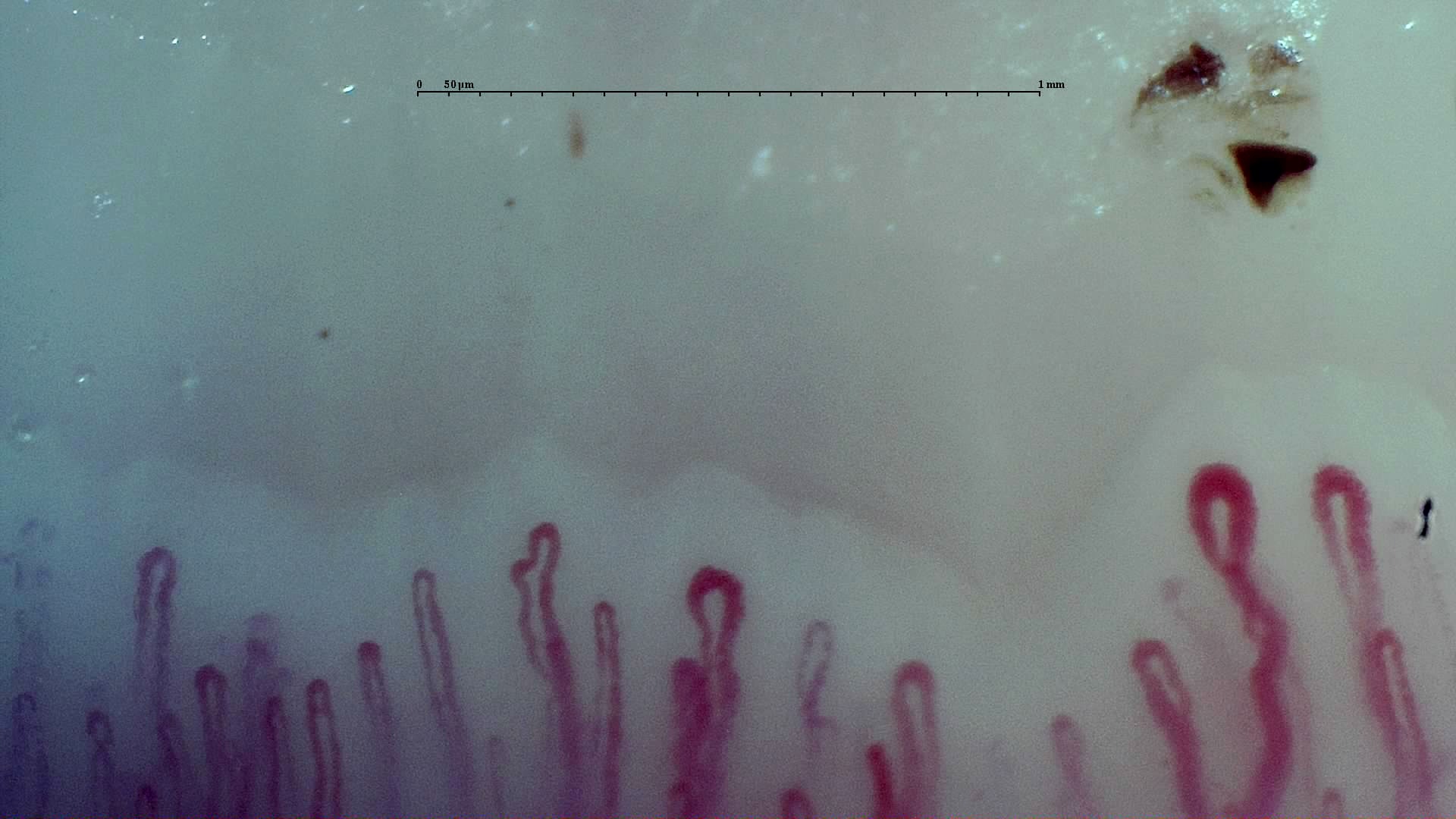 A. Early phase
A. Early phase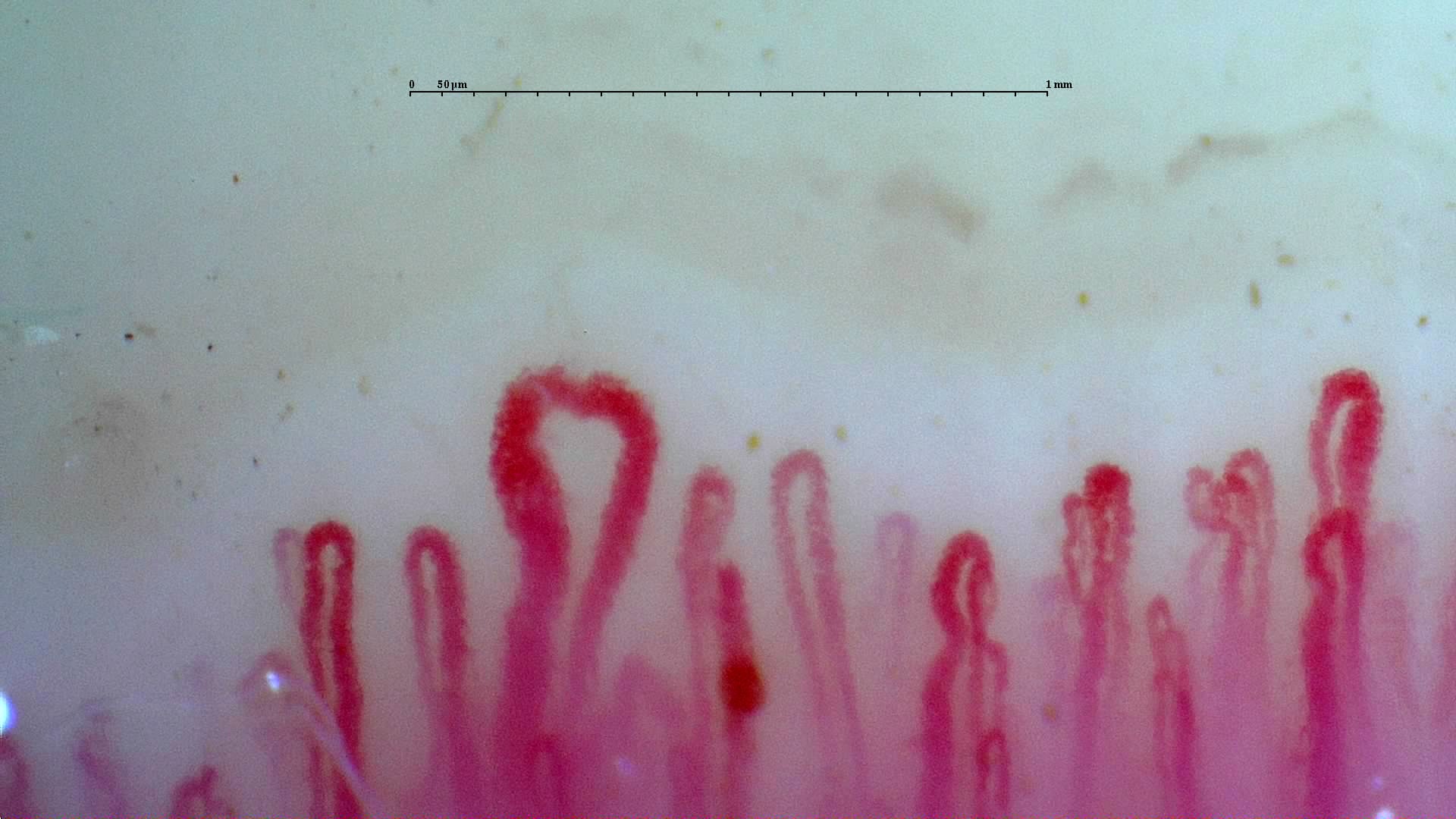 B. Active phase
B. Active phase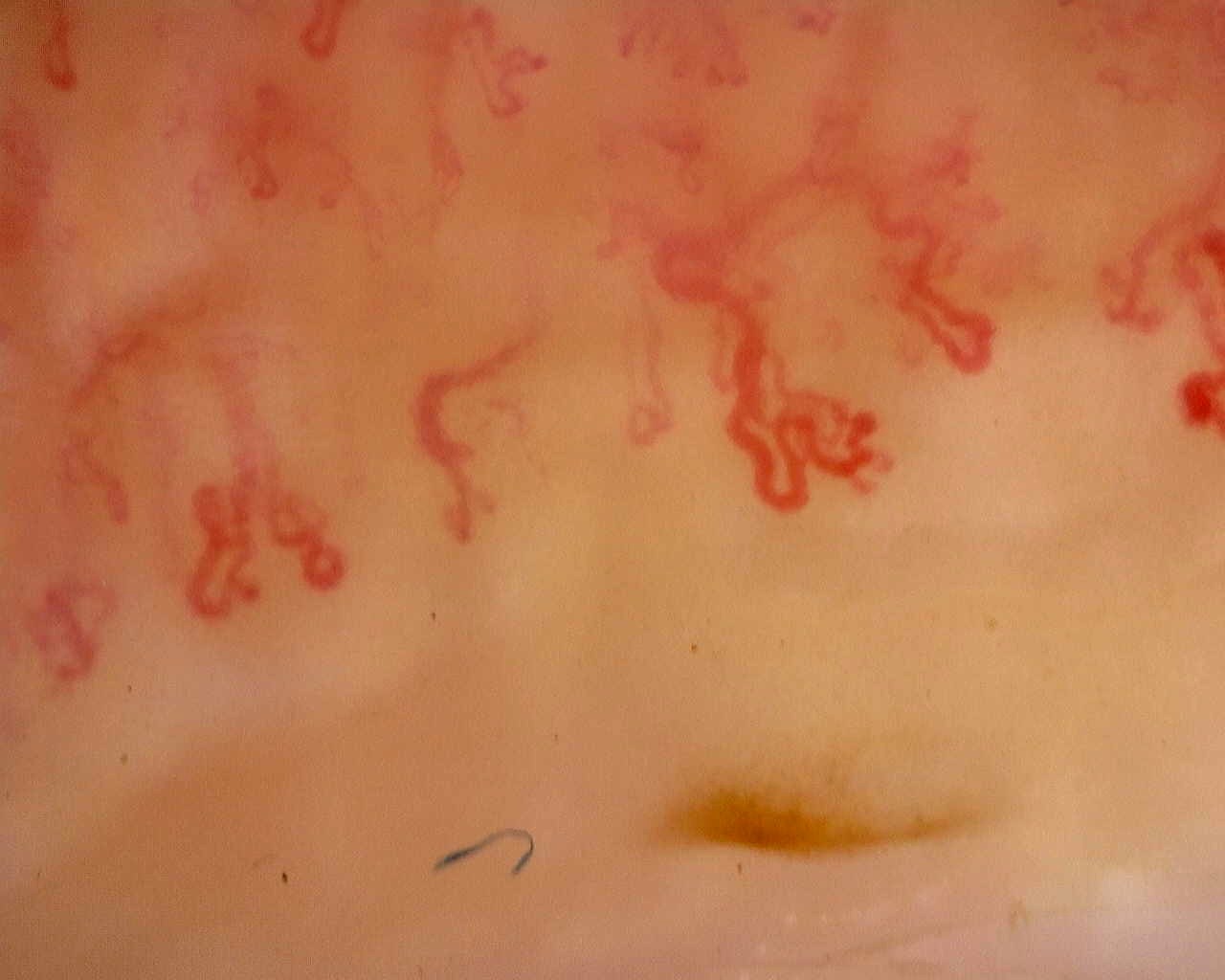 C. Late phase
C. Late phase- Repeat the test with an explicit clinical question: vascular risk, progression, or correlation with a phenotype change.
- Always compare equivalent fingers with similar technical quality [2].
- Do not take an isolated determination as a substitute for echocardiography, pulmonary function tests (PFTs), high-resolution computed tomography (HRCT), or vascular examination.
- Describe whether you detect pattern transition, additional density loss, or new avascular areas [1, 3, 14].
- If the study is not comparable because of technique or visibility, state this in the report.
Short cases
These scenarios summarize how capillaroscopy can be used during follow-up without excessive enthusiasm or unnecessary skepticism.
Case 1: recurrent ulcers and obvious rarefaction
A woman with limited systemic sclerosis, prior digital ulcers, and new density loss with avascular areas. Capillaroscopy does not replace vascular assessment, but reinforces that the microvascular phenotype is high risk and that peripheral control should be intensified [1, 4, 5, 6, 7].
Case 2: worsening pulmonary function
A patient has a drop in diffusing capacity for carbon monoxide (DLCO) and capillaroscopy evolving from active to late pattern. The image does not diagnose PAH or ILD, but supports systemic vasculopathic progression and should prompt complete cardiopulmonary screening [1, 9, 10, 11].
Case 3: severe pattern but stable disease
A patient has a known late pattern, no new ulcers, no functional deterioration, and no skin progression. The finding remains important, but a new capillaroscopy only makes sense if it adds information that changes management. Repeating by inertia adds less than contextualizing it with the rest of follow-up [1, 2].
FAQ
Which clinical event is best supported by capillaroscopy prognostically?
Peripheral vascular risk, particularly digital ulcers, where capillary loss and late pattern show the most consistent association [1, 4, 5, 6, 7, 14].
Does CSURI work in every patient with systemic sclerosis?
No. It is useful in some subgroups, but it is not always calculable and its real-practice performance has been lower than in initial studies [5, 6].
Does severe capillaroscopy necessarily imply worse survival?
Not necessarily as an independent factor. It is usually associated with a more severe phenotype, but part of the association may be explained by cutaneous subtype, ILD, PAH, or other covariates [8, 13].
Can capillaroscopy replace PAH screening?
No. It can increase suspicion and enrich stratification, but it does not replace specific cardiopulmonary assessment [1, 2, 9, 10].
Glossary
- CSURI
- Capillaroscopic Skin Ulcer Risk Index, a score designed to estimate the risk of new digital ulcers in selected patients with systemic sclerosis.
- NEMO
- Index centered on hemorrhages and microthrombosis, used as a marker of microvascular activity and digital ischemic risk.
- Late pattern
- Advanced capillaroscopic phase characterized by obvious rarefaction, avascular areas, neoangiogenesis, and architectural disorganization.
- Capillary rarefaction
- Reduction in the number of visible capillaries per millimeter in the distal row, interpreted as loss of the microvascular bed.
- Hard outcome
- High-impact clinical event such as digital ulcer, pulmonary arterial hypertension, major cardiovascular event, or mortality.
References
- Smith V, Ickinger C, Hysa E, Snow M, Frech T, Sulli A, et al. Nailfold capillaroscopy. Best Pract Res Clin Rheumatol. 2023;37(1):101849. doi: 10.1016/j.berh.2023.101849. PMID: 37419757.
- Smith V, Herrick AL, Ingegnoli F, Damjanov N, De Angelis R, Denton CP, et al. Standardisation of nailfold capillaroscopy for the assessment of patients with Raynaud's phenomenon and systemic sclerosis. Autoimmun Rev. 2020;19(3):102458. doi: 10.1016/j.autrev.2020.102458. PMID: 31927087.
- Smith V, Decuman S, Sulli A, Bonroy C, Piette Y, Deschepper E, et al. Do worsening scleroderma capillaroscopic patterns predict future severe organ involvement? A pilot study. Ann Rheum Dis. 2012;71(10):1636-1639. doi: 10.1136/annrheumdis-2011-201009. PMID: 22402146.
- Boulon C, Ballerie A, Guérin C, et al. Nailfold capillaroscopy findings are associated with a history of digital ulcers in the same finger in systemic sclerosis patients: results from the SCLEROCAP study. Semin Arthritis Rheum. 2022;54:152002. doi: 10.1016/j.semarthrit.2022.152002. PMID: 35367233.
- Sebastiani M, Manfredi A, Vukatana G, Moscatelli S, Riato L, Bocci M, et al. Predictive role of capillaroscopic skin ulcer risk index in systemic sclerosis: a multicentre validation study. Ann Rheum Dis. 2012;71(1):67-70. doi: 10.1136/annrheumdis-2011-200022. PMID: 21917823.
- Walker UA, Jaeger VK, Bruppacher K, Dobrota R, Arlettaz L, Banyai M, et al. Prospective evaluation of the capillaroscopic skin ulcer risk index in systemic sclerosis patients in clinical practice: a longitudinal, multicentre study. Arthritis Res Ther. 2018;20(1):239. doi: 10.1186/s13075-018-1733-6. PMID: 30359309.
- Del Papa N, Sambataro D, Minniti A, Pignataro F, Caporali R. High NEMO score values in nailfold videocapillaroscopy are associated with the subsequent development of ischemic digital ulcers in patients with systemic sclerosis. J Rheumatol. 2020;47(9):1414-1417. doi: 10.3899/jrheum.190908. PMID: 33050944.
- Tolosa-Vilella C, Guillén-Del-Castillo A, Simeón-Aznar CP, Colunga-Argüelles D, Gallego-Bernad M, Rubio-Rivas M, et al. Late versus non-late nailfold capillaroscopic patterns in systemic sclerosis patients: A detailed analysis from the RESCLE registry. Autoimmun Rev. 2023;22(5):103310. doi: 10.1016/j.autrev.2023.103310. PMID: 37098269.
- Minopoulou I, Tentolouris A, Boulon C, Ntusi N, Tieu J, Marie I, et al. Nailfold capillaroscopy abnormalities in patients with systemic sclerosis-associated pulmonary arterial hypertension: A systematic review and meta-analysis. Microvasc Res. 2021;136:104161. doi: 10.1016/j.mvr.2021.104161. PMID: 33917407.
- De Angelis R, De Luca G, Melsens K, et al. Significant capillary loss and late nailfold capillaroscopy pattern are associated with pulmonary arterial hypertension in systemic sclerosis. Rheumatology (Oxford). 2024;63(3):783-791. doi: 10.1093/rheumatology/kead557. PMID: 37624917.
- Smith V, Ruaro B, Allanore Y, et al. Greater capillary loss associates with more severe interstitial lung disease in patients with systemic sclerosis and progressive fibrosing ILD: post-hoc analysis from the SENSCIS trial. Lancet Rheumatol. 2025;7(1):e5-e15. doi: 10.1016/S2665-9913(24)00296-0. PMID: 41107055.
- Correia AM, Ferri C, Spinella A, et al. Capillary loss and giant capillaries are associated with diffuse and limited cutaneous systemic sclerosis, respectively: a detailed analysis. Microvasc Res. 2025;167:105178. doi: 10.1016/j.mvr.2024.105178. PMID: 40617586.
- Valera-Ribera C, Guillén-Del-Castillo A, Carbonell A, López-Soto A, Rubio-Rivas M, Cases A, et al. Digital vasculopathy and avascular scores in nailfold videocapillaroscopy as a predictor of major cardiovascular events and mortality in systemic sclerosis. Rheumatology (Oxford). 2025;64(1):233-242. doi: 10.1093/rheumatology/keae240. PMID: 41076942.
- Boulon C, Larrouture I, Blaise S, Mangin M, Decamps-Le Chevoir J, Senet P, et al. Nailfold video capillaroscopy predicts severe progression at three years in systemic sclerosis: Results from SCLEROCAP study. Microvasc Res. 2026 Jan;163:104874. doi: 10.1016/j.mvr.2025.104874. PMID: 40967366.